The Win-Win Potential of Hiring Neurodiverse Workers

The Win-Win Potential of Hiring Neurodiverse Workers
Sap Insights, 2019
With the right hiring approach and on-the-job supports, people with developmental differences can contribute valuable talents and achieve important payoffs for their organizations.
In 2019, Nicolas (Nico) Neumann was the first individual to take home SAP’s most prestigious employee award. Created in 2014, the Hasso Plattner Founders’ Award had in the past gone to multimember teams for inventions such as creating an immersive customer experience and a zero-downtime software upgrade option. Neumann won for creating a tool to automate complex cross-company invoices, reducing a process that took at least two days to one that took 20 minutes.
SAP’s financial accounting department implemented the tool. And the difference it made led to Neumann’s recognition.
It was “great to see how a single human being with just a simple idea but a great drive to achieve it can really change the world,” says Luka Mucic, SAP’s chief financial officer.
Neumann joined SAP Argentina in 2016 through the Autism at Work program, which supports candidates on the autism spectrum during the hiring process and offers a variety of resources once they’re hired.
Not every neurodivergent employee your company brings on board will achieve such a breakout accomplishment. The neurodiverse – like the neurotypical – are, as the term suggests, diverse. Neurodivergent people are often fully aware of their strengths and gaps that allow them to reach their full potential. As with all employees in every organization, their skills, capabilities, and potential vary.
This recognition makes it important for employers developing hiring programs that welcome the neurodiverse and people with disabilities to start with an emphasis on allowing individuals to bring their whole selves to work. This allows them to reach their potential and allows the hiring organizations to capture the valuable skills and perspectives that they offer. These programs design career pathways for individuals to participate as much as possible, with as few limitations as possible, by providing accommodations in every aspect of employment throughout their tenure.
Successful programs designed to employ neurodiverse candidates raise awareness among employees of the effort and make important alterations to the recruiting and onboarding processes as well as adaptations to communications and management approaches.
The investment is worth it as companies benefit from the achievements, skills, experiences, and unique perspectives of individuals they might otherwise overlook. Because when organizations fail to see what individuals have to offer – through misconceptions, bias, or some other factor – it is a missed opportunity.

An overlooked talent pool
At a time when a range of industries, such as food services and IT organizations, are facing rafts of open positions, neurodiverse candidates who have historically been overlooked during the hiring process can represent great potential.
A disability has three dimensions, according to the World Health Organization definition: impairment, such as physical or mental function; activity limitation, such as hearing, seeing, or problem-solving; and participation restrictions, whether in work, recreational activities, or receiving healthcare. About 15% of the world’s population has a disability.
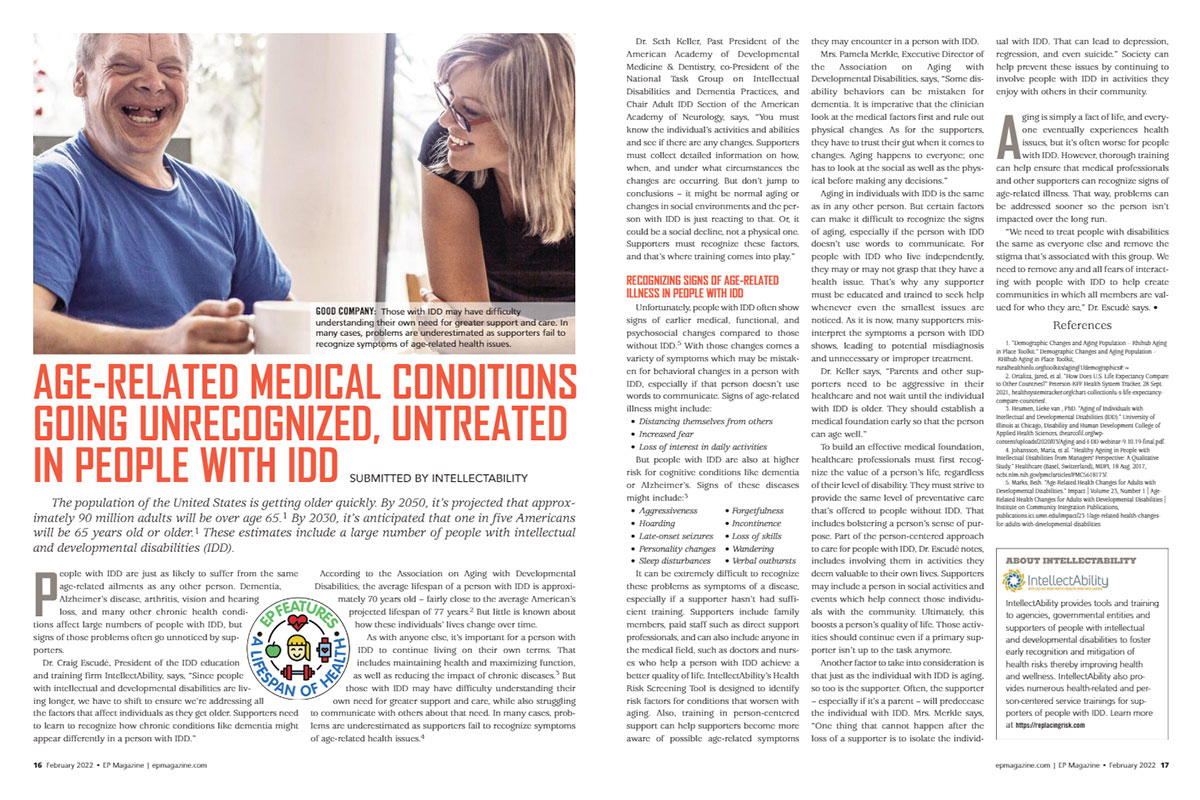
“Unfortunately, many businesses and employers are reluctant to hire these individuals, even though, in many cases, they perform as well or even better than other employees.”
Craig Escudé, President of IntellectAbility
People with disabilities are underemployed. In 2021 in the United States, for example, only 19% of people with a disability were employed, according to the Bureau of Labor Statistics. This population includes people with physical limitations as well as intellectual and developmental disabilities (IDD). And while the employment base for disabled Americans rose slightly from the 17.9% level recorded in 2020, it lagged far behind the 63.7% of people without a disability who were employed in 2021.
“Unfortunately, many businesses and employers are reluctant to hire these individuals, even though, in many cases, they perform as well or even better than other employees,” says Craig Escudé, a family physician and president of IntellectAbility, an organization that educates families and service providers who support people with intellectual disabilities.
Escudé says that a notable research study found that employers overlook people with intellectual or developmental disabilities for a range of reasons that go beyond negative stereotypes, including concerns about coworkers’ and customers’ negative reactions; assumptions that it will cost more to hire, train, and retain people with IDD and that these workers won’t be as productive; and fear of litigation associated with the hiring and firing of people with disabilities.
While research data during the pandemic is scant, there is evidence that an inclusive recruiting approach can pay off. A 2018 study by Accenture, Disability:IN, and the American Association for People with Disabilities found that in a sample of 140 U.S. companies, the 45 that actively pursued hiring people with disabilities performed better in terms of revenue and net income.
In addition, the labor market in 2022 is creating a win-win for those with disabilities as well as for older workers, says Richard Wahlquist, CEO of the American Staffing Association, a trade group. “It’s the best time in my 30 years in the industry for older workers and people with disabilities, and our industry is looking for them,” Wahlquist says.
It’s not enough, though, to have the desire to reach out to the neurodiverse population as a potential talent pool. The culture and climate of the organization must support such efforts.

People with the power to contribute
Jim Hogan is an accomplished technology executive who is autistic.
Diagnosed when he was four years old, Hogan, who is now 55, describes himself as “a dedicated lifelong autodidact” who turned some of that self-teaching to computer science. Before joining Google in mid-2020, Hogan had technology management and director roles at companies including Accenture, Verizon, Kaiser Permanente, and Genesys. At Google, he has more than one role: he serves as principal innovation strategist, healthcare and life sciences, and as vice president of accessibility in technology. (To make things interesting, he has been studying immunology through Harvard Medical School’s HMX online program.) Hogan’s LinkedIn profile notes that he is “an innovator, a human rights activist, and a strong representative of what is possible for autistic individuals.”
Hogan knows how challenging the employment landscape can be for those on the autism spectrum based on his own experience of being a victim of bullying over the years from coworkers and managers. In 2004, a peer subjected him to what he calls “widespread public humiliation, making up lies about situations that never took place to ruin my credibility, and general cruelty.” The bullying progressed to the point, he says, of a complete psychotic break. He was hospitalized for over two weeks.
“I have found a belonging here that has eluded me for my entire career.”
Jim Hogan, Principal Innovation Strategist and Vice President, Google
Now thriving, Hogan says his career experience also shows how energizing it can be to find the right employer and role. Soon after he joined the company, he was asked to help Google Cloud institute an autism hiring program. His initial response: “Don’t do us any favors.”
Hogan says he pointed out that it’s not just about filling the hiring funnel with a certain type of individual but about bringing people into an organization that is ready for them. The culture and climate must be supportive.
With Hogan’s help, Google sought input from other autistic employees and the Stanford Neurodiversity Project, which advises employers on improving these workers’ on-the-job experiences. An estimated 500 Google Cloud managers received training on effective hiring and onboarding practices for neurodiverse candidates. Google Cloud launched its Autism Career Program in July 2021, with Stanford providing ongoing coaching and support for applicants and their Google teammates and managers – steps designed to ensure a supportive culture for neurodiverse candidates.
Hogan says his employer encourages him to follow his passions, both as a technologist and as an advocate for others. “I feel connected with Google in my favorite causes such as innovation evangelism, accessibility for everyone, and trying to make work environments psychologically safe for everyone. I have found a belonging here that has eluded me for my entire career,” he says.

Actions on the road to inclusion
Hogan and Neumann represent top performers who happen to be neurodivergent. But they wouldn’t be in their positions to make significant contributions if their organizations did not have cultures in which they could thrive and systems in place to support them.
These elements don’t appear fully formed in an instant, says Anu Mandapati, chief diversity, equity, and inclusion (DEI) officer at consultancy IMPACT Leadership Partners in Austin, Texas. “The biggest thing about DEI is that it’s a journey. It’s not about perfection; it’s about practice. The more you practice, the better you’ll get. That’s when we become confident as a company,” Mandapati says.
Steps organizations can take include:
Train everyone from top to bottom to accept individuals’ differences.
Offer awareness sessions to help employees understand the different perspectives that people who have IDD may bring to the workplace – and the supports the organization provides. Make everyone aware that they are participating in a broader effort that covers a range of settings – including the hiring and onboarding process and everyday interactions – and that this effort belongs to everyone, not just those in HR.
Leaders should participate, too, says Tova Sherman, CEO of reachAbility Association, a nonprofit based in Halifax, Nova Scotia that consults and trains with organizations building DEI programs. “If you send your employees to training related to inclusion and hiring people with disabilities, you, as the leader, need to be at that training,” Sherman says.
Ease the pressure during hiring.
The interview process can be extremely challenging for neurodivergent candidates, hindering their ability to adequately convey their aptitude and competencies. Finding ways to relieve stressful situations can make a meaningful difference. Productive moves that HR professionals and employees cite include:
Training for interviewers. Interviewers can receive coaching to minimize unconscious bias they might bring to meetings with candidates who have disabilities. For example, every interviewer in the Google Cloud program is trained to recognize and move beyond tendencies that are exclusive or that lack awareness and understanding, Hogan says.
Specialized skills assessments can take the place of interviews to evaluate a candidate’s competence for certain types of roles. Microsoft’s neurodiversity hiring program starts a candidate off with an online technical assessment before inviting them to an event that includes spending a few days on technical skills, team-building, and interview preparation.
Do-the-work tryouts instead of interviews. SAP’s Autism at Work program, which launched in 2013 and now has 215 employees in 16 countries, provides an illustrative example here.
When Carrie Hall, who is autistic, joined the Autism at Work program in 2015, she says the hiring process had marked differences. Instead of facing a battery of conceptual interview questions that she might find ambiguous or unclear, Hall was invited to perform sample work tasks for about a week so that she could demonstrate her ability to do the job. Today, Hall is in her second job at SAP, as a senior product inclusion specialist. It’s a position she calls her dream job, working in a team on inclusive product design and accessibility.
Hall says the initial opportunity for candidates like her to perform work is instrumental. It helps others get a sense of the candidates’ potential, while candidates also get a sense for the work, the people, and whether the place is a good fit for them.
Coaches for job candidates. Offering accommodations for interviewees that need them is another important best practice. At SAP, for instance, those applying through the Autism at Work program may seek assistance through accommodated interviews that might involve a job coach before, and even during, the interview.
Build awareness of available supports during on boarding.
For employees on the autism spectrum, the onboarding period offers an opportunity to learn about the supports that are available to them. These could include (as with the Autism at Work program) introductions to workplace mentors and access to life skills assistance, such as finding an apartment or arranging transportation. It could mean in-office accommodations, such as quiet spaces with limited distractions, a comfortable chair, a preferred style of lighting, or requests for their attention previewed in an e-mail instead of a spontaneous comment over the cubicle wall.
Mike Giongo is a process management specialist on the SAP Global Strategy & Insight team. He came to his role from the Autism at Work program, where he started as an intern in 2015 through a referral from the Pennsylvania Office of Vocational Rehabilitation after his college graduation.
Giongo says active coaching throughout the onboarding process was important to his success. “It’s got to be organized. It’s got to be persistent. It’s got to be consistent, and expectations have to be clear and clearly communicated on both ends,” he says. “Onboarding can be like navigating a maze and can become stressful very easily,” he says.
Provide ongoing support to retain talented people.
The supports shouldn’t stop once the formal onboarding process is over. Retaining neurodiverse employees requires ongoing attention throughout their tenures with their organizations. Communication preferences tailored to individuals and peer mentors provided to employees on the autism spectrum are two examples.
Communication preferences are very important to consider because based on a person’s ability to express and receive information, the means of sharing ideas can help or hinder a person’s ability to work with colleagues, says Google’s Hogan. Some people prefer in-person conversations; others might need to read an e-mail instead to get the meaning. To accommodate this need, Google has introduced “user guides” connected to employee profiles that indicate a person’s communication preferences. It’s simple, effective, and personalized.
Communication preferences are very important to consider… Some people prefer in-person conversations; others might need to read an e-mail instead to get the meaning.
Peer mentors are another example. SAP’s Hall points to two mentors that helped her with her resume and interview prep – one neurotypical and the other autistic. Hall’s neurotypical mentor, a user experience designer, encouraged her to apply for positions at SAP and helped her redo her resume so that it conveyed her background and experience in ways that aligned with the requirements of the position she sought. Another autistic employee, a data scientist, helped her with interview prep and understanding job descriptions, which can be challenging for someone who is autistic, Hall says.
“He’s a data scientist who was able to see patterns in the job description and could identify what I could focus on for the interview,” Hall says.
This mentor’s support was notable; Hall says she strongly believes that autistic individuals can serve as strong mentors for others who may have different life or career experiences. She started a nonprofit group, Autistic Women’s Alliance, to support diagnosed or self-identified autistic women in their careers. The focus on women is important because women tend to be diagnosed later than men, Hall says.
Job applications are one area in which support can help. Another is resumes.
Based on his experiences, Giongo stresses that employers should not look for a “perfect fit.” He advises not placing too much emphasis on the resume and instead considering possibilities of growth and upward mobility or other opportunities in the organization. Considering different approaches can help both employees and organizations find the right fit.

Recognize: You’re dealing with individuals, not “types”
A common saying in autism circles is, “When you’ve met one person with autism, you’ve met one person with autism.” It’s a recognition that every individual has traits that make them unique. The same is arguably true when meeting people of any kind, regardless of their abilities.
Giongo, the project management specialist who joined SAP full-time in 2018 after an internship from 2015 to 2017, says his current job has challenged him intellectually and socially, pushing him beyond his comfort zone – a good thing – but always with guardrails provided by the company. “I was consistently challenged, but I was never made to feel uncomfortable,” he says.
This balance – challenges with supports – has helped Giongo meet his responsibilities. And he thinks it shows how a company doesn’t need to seek out a perfect fit for every position. Organizations can, he says, “account for the fact that the needs of all individuals are in a persistent state of evolution, especially in the workplace, and to calibrate communications accordingly.”
At the beginning of this article, if we hadn’t told you that Nico Neumann was a neurodivergent employee and part of SAP’s Autism at Work program, you probably would have focused on his award-winning invention for invoicing.
That’s as it should be. The point at which we no longer need to identify employees as having a disability is really the point we should strive for. In the meantime, to achieve the goal of offering everyone more opportunities so that organizations can gain access to the broadest array of talent means we do need to focus specifically on those who have IDD and other disabilities.
Once they’re in the workplace, though, what matters most isn’t who they are or the labels used to define them, but what they do – their contributions. And those contributions can be significant.
Feature originally published by SAP.