Validated & Reliable
Predictor of Mortality

Validated Against Real Outcomes
The Health Risk Screening Tool (HRST®) is not a documentation system, and it is not a general-purpose electronic health record. It is a validated health risk screening and stratification instrument designed to identify people at elevated risk, quantify the severity of that risk, and support timely intervention before destabilization becomes a crisis.
Independent research, peer-reviewed publication, and multi-year state-level analyses all point to the same conclusion: the HRST identifies clinically meaningful risk that correlates with real outcomes, including adverse events, healthcare utilization, and mortality.¹ ²
The HRST identifies risk, stratifies that risk into actionable Health Care Levels (HCL), and supports interventions aimed at preventing escalation. That progression, from identification to stratification to intervention to prevention, is what makes the HRST fundamentally different from systems that only document information after the fact.
Predictive Validity Supported by Independent Analysis
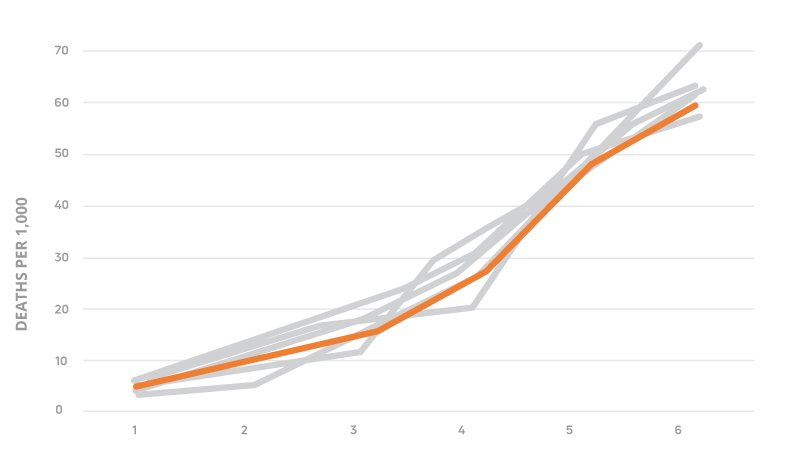

Mortality rates increase consistently with higher HRST Health Care Levels across multiple state datasets, demonstrating a clear relationship between risk stratification and real-world outcomes.²
Across large-scale analyses of people with intellectual and developmental disabilities, higher HRST Health Care Levels have been consistently associated with significantly higher mortality rates.¹ ² This relationship has been observed across multiple independent analyses and state-level datasets, demonstrating that HRST risk stratification reflects real-world clinical vulnerability.
Peer-reviewed research published in the Journal of Nursing Measurement further confirmed the HRST’s predictive validity in a sample of more than 12,500 people with IDD, demonstrating that Health Care Levels are predictive of mortality and can serve as a basis for establishing healthcare needs and determining nursing care acuity.¹ The significance of that finding is straightforward: HRST scores are not abstract ratings. They correspond to real differences in vulnerability, clinical need, and outcome risk.
State-level analyses add another important layer of evidence. Across multiple years of mortality reporting, elevated HRST risk has been consistently associated with increased likelihood of death, while related analyses have also shown that elevated risk is associated with increased likelihood of adverse events, including hospitalizations and emergency department utilization.² Additional state-level analysis has demonstrated that elevated HRST risk is associated with increased hospital and emergency department utilization, and that coordinated system responses can resolve and mitigate these events.³ Taken together, these findings show that the HRST does more than describe risk. It identifies risk in a way that is predictive, actionable, and operationally relevant.
Journal of Nursing Measurement
The HRST can predict mortality. Therefore, it can serve as a basis for establishing healthcare needs and determining nursing care acuity."
- Journal of Nursing Measurement, Vol. 28, No. 1, April 2020
This peer-reviewed study analyzed data from more than 12,500 people with intellectual and developmental disabilities and found a clear, consistent relationship between HRST Health Care Levels and mortality outcomes. As risk levels increased, so did the likelihood of death, demonstrating that HRST stratification reflects real-world clinical risk at scale.¹
Real-World Evidence Beyond Mortality
The HRST’s value is also reflected in real-world implementation outcomes.
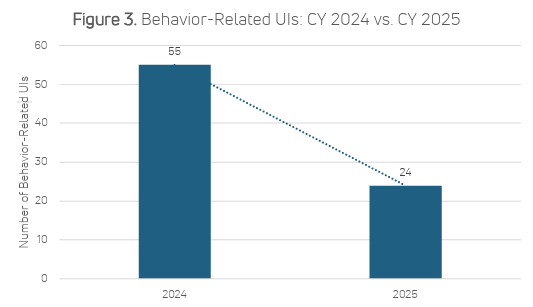
Provider-based outcome studies have shown measurable reductions in emergency department visits, hospitalizations, falls, behavior-related crises, and other destabilizing events following HRST implementation.⁴ ⁵ In one provider study, implementation was associated with a 50% reduction in unanticipated hospitalizations, a 43% reduction in emergency department visits, and estimated direct medical cost avoidance exceeding $136,000.⁴ Additionally, behavior-related unusual incidents, defined as peer-to-peer aggression, self-injurious behavior (SIB), or destruction of property, declined by 56% following HRST implementation.
In another case study, implementation was associated with a 20% decrease in preventable healthcare medications, a 25% reduction in falls, and improvement in Health Care Level for 10% of people supported.⁵
These outcome studies are important because they complete the full continuum of evidence. The HRST identifies risk, that risk correlates with real adverse outcomes, and use of that information supports earlier intervention and reduced escalation.
Independent Reliability Supports Consistency
A risk screening instrument must also be dependable in its application. Independent reliability analysis using a large dataset found good internal consistency and very strong test-retest reliability over time, supporting the stability and consistency of HRST scoring in real-world use.⁶
Validity depends on consistency. The HRST is not only predictive. It is structured to produce reliable, repeatable results across large systems.
Translating Risk into Action at the System Level
A validated risk stratification system must do more than generate scores. It must enable organizations to identify who is most vulnerable, determine where clinical attention is required, and intervene before unmanaged risk results in avoidable suffering, unnecessary utilization, or premature death.
The HRST translates observed risk into structured Health Care Levels and associated Service and Training Considerations, enabling earlier recognition of destabilization, more targeted clinical involvement, and more appropriate oversight at the system level. This allows organizations to move from reactive crisis response to proactive health management.
For state Medicaid agencies, state DD divisions, and managed care organizations, this supports stronger clinical oversight, acuity-informed planning, more precise resource deployment, improved cost management, and greater accountability for outcomes.