Gastroesophageal Reflux
Recognizing the Enemy is Half the Battle!
In last month’s newsletter we addressed The Fatal Five; the top five killers of people in both in both institutional and community settings. Over the next several months we would like to discuss each of them individually. This month we will be discussing GERD and how to recognize it in its many forms. When left untreated, not only is reflux extremely uncomfortable but it can lead to death from frank aspiration, GI bleed or esophageal cancer.
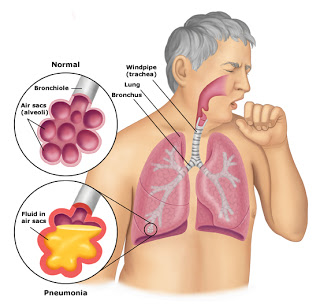
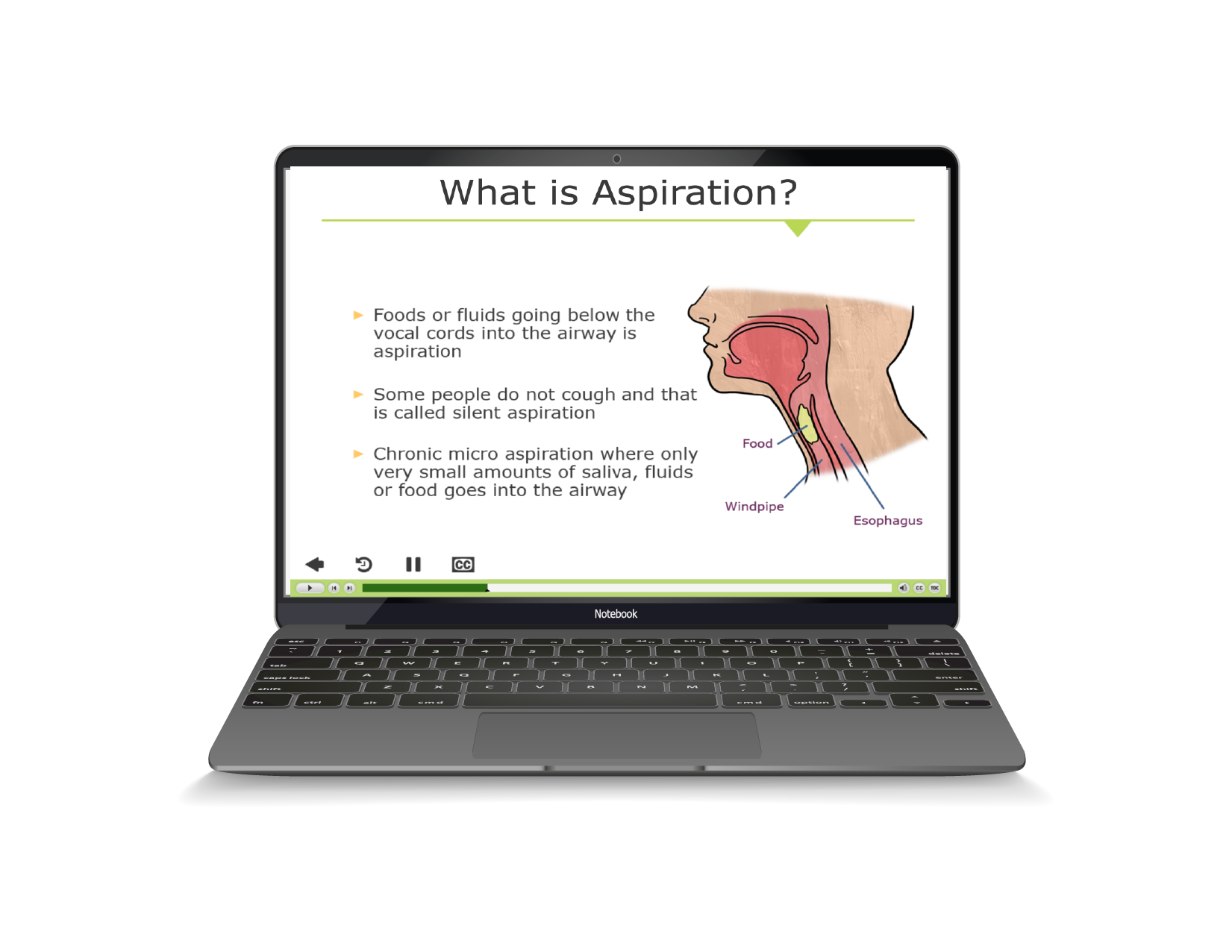
Gastroesophageal reflux disease or GERD is the reverse flow of stomach contents into the esophagus. Once outside the protected environment of the stomach, stomach acid can irritate and harm the esophagus, be inhaled or aspirated into the lungs, or damage the gums and teeth.
GERD is often nature’s way of telling us that our diet needs some attention. Foods that contain acid (tomatoes, citrus) excessive fats, coffee, alcohol, spicy foods, chocolate and mint may cause or worsen reflux. Carrying excessive weight, particularly around the abdomen, can exacerbate the symptoms of reflux, both due to lack of tone of the abdominal muscles and the mechanical pressure of the excess mass exerting upward pressure on the stomach and its contents.
Train those who work and live with vulnerable individuals to recognize and report the signs and symptoms of gastrointestinal disorders at the earliest possible time.
Individuals who have chronic health issues have an increased vulnerability to GERD. Other factors that can contribute to the development of reflux include significant physical disability (especially those that alter the anatomy of the GI tract), hiatal hernia, emotional and behavioral issues, tube feeding diets and, above all, medications (anticholinergics, muscle-relaxers, NSAIDS and MANY others.) Fortunately there are several easily recognizable factors that can indicate that a person has or is likely to develop reflux.
Common signs of reflux are burning pain in the upper abdominal or chest areas, regurgitation of stomach contents, meal refusal, belching and/or flatulence. Less commonly seen are behavioral signs such as hand-mouthing and PICA which, when present, have a 30% correlation with silent reflux. Other symptoms of silent reflux are unexplained weight loss, low serum albumin and progressive anemia.
Medications have been the most commonly used first line of defense against GERD. Proton pump inhibitors such as Prilosec (omeprazole) and Histamine-2 antagonists like Zantac (ranitidine) are frequently used. Problems with these medications include malabsorption of vitamin B-12 and protein. Fractures associated with impaired calcium absorption are also requently seen with long-term use.
Other steps that can be taken to combat reflux include:
- Maintain a proper body weight for height.
- Consume a well-balanced diet in reasonable portions three or more hours prior to bedtime.
- Avoid foods that are known to aggravate heartburn, keeping in mind that everyone benefits from the occasional indiscretion, especially those that are covered in chocolate.
- Identify medications that are associated with GI distress and discuss symptoms with the prescribing physician so that these are used only when absolutely necessary.
- Identify and use positions that promote emptying of the stomach.
- Promote the swallowing of saliva, which neutralizes acidic stomach contents by having individuals who drool evaluated and treated by a speech pathologist.
- Train those who work and live with vulnerable individuals to recognize and report the signs and symptoms of gastrointestinal disorders at the earliest possible time.
Gastrointestinal Rating Information for HRST Users
“Has this person shown signs or symptoms of GI problems, including behavioral signs, within the past year OR had a gastrointestinal bleed at ANY time in their life?”
This is the opening rating question for Item K. Gastrointestinal on the HRST. Any and all conditions affecting the GI tract are rated in this section, but please be aware that we do not wait for the physician to grant a diagnosis in order to score this item. Gastrointestinal issues are some of the most pervasive and under-diagnosed health problems in the world. They may only become evident when the person has experienced some kind of a crisis such as a gastrointestinal bleed or an aspiration event.
Important things to look for in the individuals you serve are food aversions or avoidance, excessive belching, heartburn, rumination, unexplained vomiting, appearance of ingested food, including feeding tube formula, in the back of the throat, coughing within three hours of meals or at night, hand-mouthing or PICA behaviors and unexplained or escalating behavioral issues. Above all, INQUIRE ABOUT THE USE OF OVER-THE-COUNTER MEDICATIONS FOR HEARTBURN, NAUSEA OR OTHER GI ISSUES!
If any of the above conditions or any other signs of possible GI issues have been observed in the past twelve months, answer YES to the first rating question on Rating Item K.
Gastrointestinal issues, once detected, are often easily treated. In almost all cases the earlier an issue is caught the fewer long term consequences will result, resulting in a happier person with a much better outlook in terms of their overall health and quality of life.